Need Assistance? Call us today! 602-478-9713

When considering technologies for home sleep testing (HST) it is important to consider that in addition to the diagnostic quality the most important variable is that the study will be self administered by the patient. In my opinion this makes Respiratory inductance plethysmography an indispensible component to a successful HST program.
The question I am most often asked about RIP is usually rooted in how RIP flow signals compare to actual respiratory flow signals acquired by a calibrated pneumotach. I have attached an overview of the history and basic science of Respiratory Inductance Plethysmography in the .ppt I presented to the American Sleep and Breathing Academy Study Club below:

Home sleep test with Nox T3 and ApneaRx
Nox Medical has continued to raise the bar in home sleep diagnostics with the Nox T3 by Carefusion. Respiratory Inductance Plethysmography is a key component in this device. The benefit of RIP is also the ease of use for the patient. Simple application of 2 effort belts will provide redundancy with the pneumotach and/or thermistor. Should the patient have the nasal sensor fall off the RIP signal can be used to reference the study post acquisition.
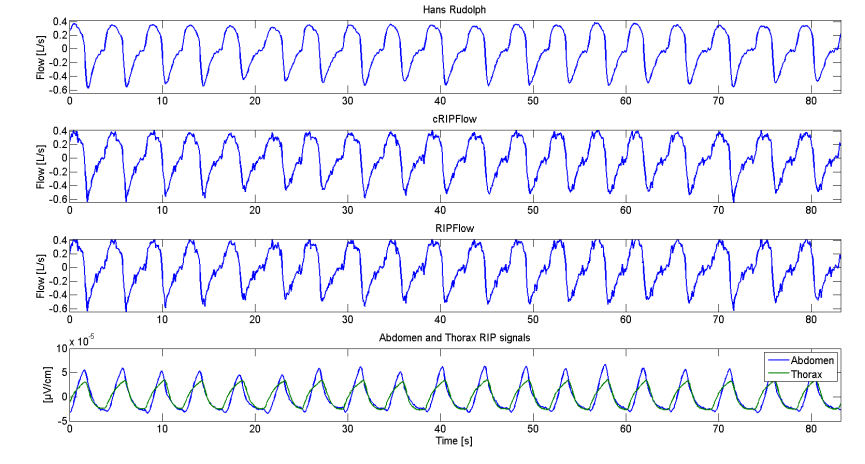
The flow measured by a Hans Rudolph pneumotach, the cRIPFlow, the RIPFlow and RIP abdomen and thorax signals during normal breathing. The total duration is 74.7 seconds. The correlation coefficient between cRIPFlow and Hans Rudolph is r = 0.994 and between RIPFlow and Hans Rudolph, r = 0.992
Hypopnea
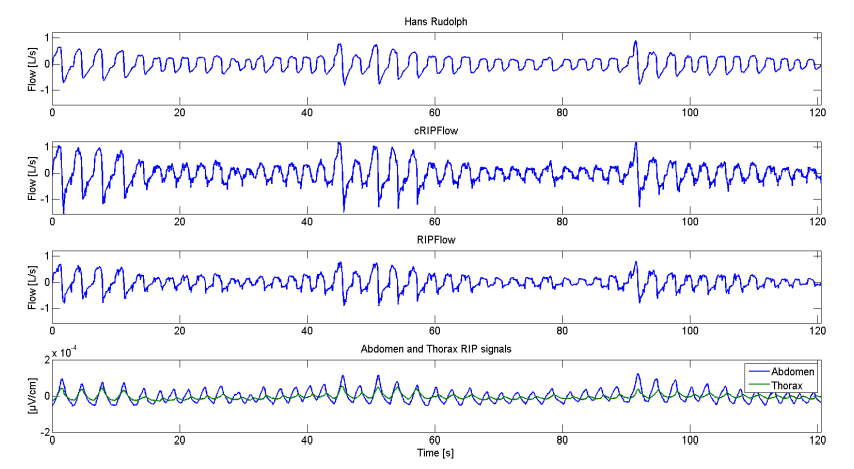
The flow measured by a Hans Rudolph pneumotach, the cRIPFlow, the RIPFlow and RIP abdomen and thorax signals during two hypopneas. The total duration is 126.8 seconds. The correlation coefficient between cRIPFlow and Hans Rudolph is r = 0.938 and between RIPFlow and Hans Rudolph, r = 0.961
Central Apnea
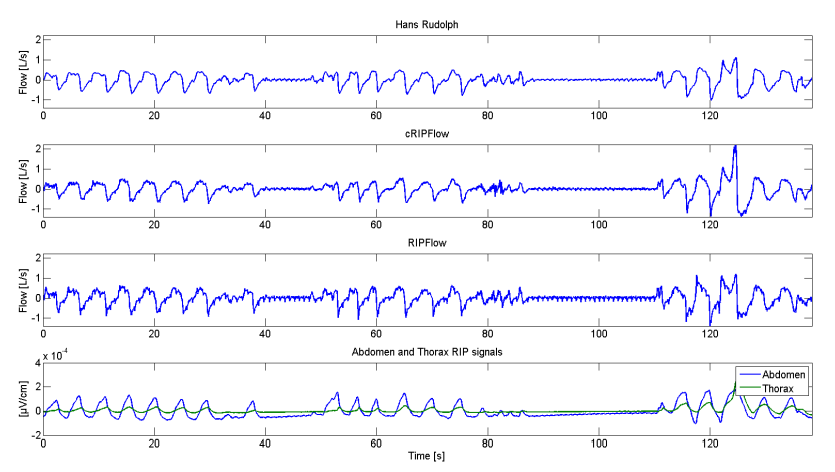
The flow measured by a Hans Rudolph pneumotach, the cRIPFlow, RIPFlow and RIP abdomen and thorax signals during two central apneas. The total duration is 126.7 seconds. The correlation coefficient between cRIPFlow and Hans Rudolph is r = 0.949 and between RIPFlow and Hans Rudolph, r = 0.927
The cRIPFlow can be used to distinguish between normal breathing, hypopneas, and central apneas as a pneumotach flow measurement.