Need Assistance? Call us today! 602-478-9713

Timothy C. Adams DDS, D. ASBA, D. ACSDD
Abstract
The Ricketts oral appliance (referred to as the Cricket Appliance), rooted in Dr. Robert M. Ricketts’ bioprogressive orthodontic philosophy, exemplifies a holistic approach to craniofacial treatment. This paper presents a comprehensive review of the Cricket appliance’s clinical applications and theoretical underpinnings, integrating advanced concepts from epigenetics and mechanobiology to quantum biology, biotensegrity, fascial dynamics, mechanotransduction, cranial bone posture, airway physiology, neurobiology, and facial asymmetry. High-quality evidence from dentistry, medicine, and biological science is synthesized and distilled to demonstrate how the appliance’s function can influence gene expression, craniofacial growth, airway dimensions, and neurology in an irrefutably logical manner. The Cricket appliance emerges as more than a tooth-moving device: it is a catalyst for orthopedic change that resonates with the body’s integrated fascial systems. By uniting interdisciplinary science with clinical precision, this work reinforces the appliance’s role in promoting balanced craniofacial symmetry, airway health, and improved neurologic development and function. Treating the root cause instead of just the symptoms is what this appliance brings to the healthcare arena like no other appliance does.
Introduction
The stomatognathic (oral-facial) complex functions as a highly integrated system that contributes not only to mastication but also to breathing, swallowing, chewing, and even neurological behaviors.¹ Pioneers like Dr. Robert M. Ricketts recognized that dentofacial orthopedics must work and be governed “by the rules of nature,” acknowledging the interplay between craniofacial structures and the rest of the body, thus reinforcing my clinical treatment syntax of posture dictates airway and neurology.¹, ², 35 The Cricket oral appliance encompasses the device and techniques developed and inspired by Ricketts’ philosophy, which was designed to guide jaw growth and tooth position in harmony with biological principles. Ricketts emphasized light, continuous forces and functional orthopedics, aiming to alter the environment of the jaws to encourage natural adaptive growth. ³, ⁵ This was an early introduction to epigenetics before it caught on in the scientific community. In contrast to heavy-force techniques that “force teeth to positions desired and dictated by the operator,” Ricketts’ methods used lighter forces that permit the arches to adapt to individual tissues.⁵ This gentle, natural, and biologically body-friendly approach is consistent with modern insights into the body’s adaptive capacity, including concepts like quantum physics, epigenetic responsiveness, mechanotransduction, biotensegrity and myofascial integration.⁶, ⁸
Purpose and Scope
In this review, we explore the Cricket oral appliance through multiple advanced scientific concepts. We first outline the appliance’s design and conventional clinical use. Then, in successive sections, we integrate eight interdisciplinary concepts – epigenetics, quantum biology, biotensegrity, fascial dynamics, cranial bone posture, airway influence, neurological signaling, and facial asymmetry – explaining how each relates to the appliance’s mechanism of action. We draw on peer-reviewed literature from orthodontics, craniofacial biology, and systems science to ensure each link is evidence-based and precise. ¹, ⁶, ⁸
Background: The Cricket Appliance and Bioprogressive Philosophy
Design and Function
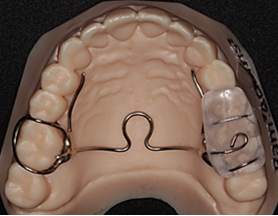
The term Ricketts oral appliance generally refers to devices stemming from Ricketts’ Bioprogressive Therapy principles. We will focus on the Cricket and the new Open Loop Cricket (OLC). 35 (figures 1,2) Ricketts advocated early intervention in growing patients, using appliances to develop arch form, enhance tongue position, improve airway, enhance cranial posture, neurology and ultimately to improve occlusal relationships. ³, ⁵ He emphasized that slow, continuous development “tends to widen the nasal cavity at a pace at which bone can fill in,” avoiding traumatic suture splitting³. In the lower arch, light forces applied via a lip bumper or utility arch could harness natural muscle pressures to distalize molars and increase arch length. ³ By releasing restrictive pressures in one area and adding gentle pressure in another, the appliance aims to direct growth and tooth eruption in a favorable manner.³ This reinforces the biotensegrity principles explained later. Removing obstacles and creating gaps and spaces is the key to giving the body the ability to heal itself.
Phonetic Bite and Mandibular Positioning
In adults, Ricketts’ principles have been adapted for oral sleep appliances. Notably, the Ricketts Phonetic Bite technique is used to register the mandible’s ideal forward position for a sleep apnea appliance⁴. In this method, the patient sits upright and repeatedly vocalizes certain sounds (counting “55… 66…” etc.) while the clinician observes vertical and anteroposterior jaw movements⁴. Specific phonetic cues – e.g., the “s” sounds in 66 and “sh” in “shun” – guide the mandible to a natural forward posture that maximizes airway patency “the individuals so called “sweet spot”.⁴ Once this position is found, a bite registration is taken with a fast-setting material to capture it.⁴ The resultant mandibular advancement device, constructed at that position, will support the jaw forward during sleep to maintain an open airway.⁴ This example underscores Ricketts’ focus on functionally derived jaw positioning – using natural functional movements (speech in this case) to determine optimal appliance positions.
Holistic Perspective
Ricketts and his contemporaries (e.g., Rudolf Slavicek) viewed the dental occlusion as part of a larger system affecting breathing, posture, neurology, and even psychological stress. ¹ They were “ready to challenge conventional knowledge” and incorporate new scientific insights into orthodontics. ¹ This progressive mindset paved the way for today’s integration of interdisciplinary concepts. Below, we delve into those concepts – epigenetic regulation, quantum-level phenomena, tensegrity-based anatomy, fascial continuity, cranial sutural biology, airway physiology, neural signaling, and asymmetry correction – and relate them back to the Ricketts appliance framework and the open loop cricket. 35
Epigenetics and the Appliance’s Gene-Environmental Interactions
Concept Overview
Epigenetics refers to heritable changes in gene expression that do not involve alterations of the DNA sequence via transduction, transcription and translation. In the context of craniofacial development, epigenetic mechanisms allow environmental signals (Quantum Physics) and functional factors to influence how genes orchestrate growth. Dental and skeletal patterns are not dictated by genes alone; rather, they result from “complex interactions between genetic, epigenetic and environmental factors” over time.⁶ For example, nutrition, muscle function, breathing patterns, chewing and oral habits can modify the expression of genes related to jaw growth and tooth development. ⁶ This means an appliance that alters functional inputs (like tongue posture or mandibular position) can trigger biological responses at the cellular level – effectively an epigenetic orthodontic effect. ⁷ ⁸
Epigenetic Orthodontics in Action
Modern clinicians have leveraged this principle with appliances designed to stimulate latent growth potential in adults. Singh and colleagues introduced the Daytime-Nighttime Appliance (DNA appliance) and coined the term “craniofacial epigenetics” for its mode of action. ⁷, ⁸ Worn only at night, the DNA appliance alters oral function (by intermittently expanding the arches and repositioning the jaw) and is hypothesized to induce a gene–environment interaction that expresses genes which had remained dormant after puberty. ⁷, ⁸ Case studies using 3D imaging found that such appliances can indeed produce increases in arch width, airway volume, and even new bone formation in sutures of non-growing adults. ⁷ The only plausible explanation for these changes in adults is the activation of gene expression (e.g., upregulating bone morphogenetic proteins or other growth factors) – an epigenetic response as Belfor noted in 2010 utilizing the Homeoblock appliance. ⁸ In essence, by changing the patient’s oral environment (jaw posture, tongue space and position, occlusal arch alignment), the appliance activates developmental pathways that in adulthood had been silenced.
Ricketts’ Environmental Paradigm
Decades before the term epigenetics was popular in dentistry, Ricketts intuitively grasped the environment’s importance. Ricketts spoke of “alteration of growth patterns” by “alteration of the environment” as a goal of treatment. ³ For instance, using a Frankel functional regulator (a tissue-borne appliance), he aimed to modify muscle forces and posture to encourage jaw growth in a favorable direction.³ Such functional appliances relieve restrictive pressures from cheeks or tongue and add new stimuli to bones and teeth, effectively remodeling the neuromuscular environment of the face. The resulting orthopedic changes – increased arch width, differential jaw growth, improved occlusion – can be seen as epigenetic outcomes because they arise from changed signals from the environment to the genome (via mechanotransductive pathways described later). A contemporary review by Brook (2009) affirms that multiple genetic pathways and epigenetic factors like local functional matrices all converge to shape dental development. ⁶ Appliances harness these principles by manipulating the functional matrix: for example, developing a narrow palate in a mouth-breather can epigenetically promote nasal breathing, which in turn can stimulate more normal maxillofacial growth patterns. ⁶
Summary
The Ricketts appliance framework aligns with epigenetic orthodontics concepts by using environmental modification as a treatment tool. It recognizes that by changing how jaws posture or how forces distribute (through an appliance via light cyclic intermittent forces), we can induce favorable gene expression changes – ultimately yielding stable orthopedic corrections rather than just transient tooth movements. ⁶, ⁸
Quantum Biology: Fundamental Biophysics of Craniofacial Change
Concept Overview: Quantum biology is an emerging field examining how quantum mechanical phenomena (such as particle-wave duality, entanglement, and tunneling) influence biological processes. 9 At first glance, quantum physics might seem far removed from dentistry and orthodontics in particular; however, biology operates at the molecular level where quantum effects are extremely impactful. For example, enzymes often rely on quantum tunneling for electron transfer, and photosynthesis efficiency is explained by quantum coherence in energy transfer. 9 In general, quantum biology explains how certain biological functions exploit quantum mechanics to achieve outcomes that classical Newtonian physics alone cannot explain. 9 These phenomena are being explored in contexts like circadian rhythm regulation, neurobiology, and DNA mutation processes.9 Understanding quantum biology encourages us to consider the craniofacial system at the most basic physical and molecular level, explaining the many dogmas that we have been taught that never made sense.
Piezoelectricity and Biophysical Signals: One strong quantifiable relationship between quantum biophysics and orthodontics is the piezoelectric property of bone and collagen. Bone is a crystalline matrix that generates electrical currents when mechanically stressed (the piezoelectric effect) – a phenomenon discovered in the 1950s by Fukada and Yasuda. Research has implicated these stress-generated electric signals in activating bone remodeling cells during orthodontic tooth movement.10 In essence, when an appliance exerts force on teeth and alveolar bone, it not only causes deformation but also produces an electrical cue that osteocytes and other cells can detect. Depending on the type of force (static or light cyclic intermittent), this electrical signal transduction operates at the interface of Newtonian and quantum physics: it involves electron movement in the bone’s crystal lattice and ion channel activation in cells, processes governed by electromagnetic and quantum principles. Orthodontic experiments have confirmed that electrically charged regions coincide with bone formation (osteoblasts) on the tension side and resorption (osteoclasts) on the pressure side of a tooth during movement.10 Thus, a Ricketts appliance subtly harnesses these biophysical cues – that apply light cyclic intermittent forces to induce an orchestrated cascade of events, from electrons to cells to proteins to tissue. The key to this cascade of events is the light cyclic intermittent forces that move with the fascia, cranial bones and cellular respiration.
Quantum Perspective on Mechanotransduction: Mechanotransduction (detailed in a later section) is fundamentally the conversion of a mechanical signal/stimulus into a biological signal. On the smallest scales, this involves proteins changing conformation, ions flowing, and even photons in some cases (e.g., light-based therapies). Quantum biology reminds us that at these scales, energy and matter behave in quantized ways. For instance, the opening of a mechanosensitive ion channel in the cell membrane (like Piezo1 in a periodontal ligament cell) might depend on the quantized energy states of that protein or the tunneling of ions through a gate. 11 While these details are still under investigation, the irrefutable logic is that biology cannot escape the laws of physics. By acknowledging quantum-level interactions, we appreciate that an orthodontic appliance’s influence permeates down to the cellular and atomic level – electrons shifting in hydroxyapatite, protons moving in collagen hydrogen bonds, etc. Notably, Melvin Moss (who developed the functional matrix hypothesis) later speculated on a “quantum biology” view of development, hinting that the very blueprint of facial growth might involve quantum processes beyond classical gene-environment paradigms.12 As Mazzoccoli (2022) describes, quantum biology provides theoretical frameworks suggesting quantum entanglement and coherence which could have functional roles in all living systems.9
Clinical Implications: In practice, dental clinicians are beginning to leverage biophysics by utilizing lasers via photobiomodulation (low-level laser or LED therapy, DEKA Lasers) to accelerate tooth movement. Photobiomodulation works by delivering photons that are absorbed by mitochondrial chromophores, enhancing cellular energy output and remodeling – a process that straddles quantum (photon absorption) and biological domains. Additionally, technologies like vibration devices apply high-frequency signals that may resonate with cellular mechanosensors, potentially influencing bone remodeling via piezoelectricity or fluid dynamics at the quantum level.13 While the Cricket appliance itself is technically a mechanical device, its optimal use may involve combining it with such modalities to maximize tissue response. The key takeaway is that on a theoretical level, appliances engage quantum-mechanical processes (even if indirectly), and future refinements in appliance therapy could involve more direct targeting of those processes (for example, appliances embedded with light sources, acrylic pads 35 or piezoelectric stimulators to encourage bone formation in specific areas).
In summary, quantum biology offers a foundational perspective reinforcing that an appliance’s effects run much deeper than visible tooth movements. They initiate a cascade of events from macro-scale force application to micro- and nano-scale events – many of which are governed by quantum laws. Recognizing this continuum enhances our precision and opens avenues for innovative, anatomical and science-based treatments, ensuring that the Cricket appliance framework and function remains aligned with the cutting edge of biological science 45 years later.
Biotensegrity: The Craniofacial Skeleton as a Tensegrity Structure
Concept Overview
Biotensegrity is a model of anatomical architecture viewing the body as a tensional- compression structure – a system of compression elements (bones, teeth) suspended in a continuous tension network (muscles, fascia, ligaments, tendons). ¹⁴ In a tensegrity structure, forces distribute optimally: when one part moves or is stressed, the entire structure rearranges tension and compression to maintain overall stability. This concept, introduced by Stephen Levin and others, provides a unifying theory for how the body maintains form and adapts to external loads. ¹⁵, ¹⁶ In the craniofacial region, biotensegrity implies that the jaw, hyoid, cranial bones, and spine form an interconnected scaffold via soft tissues. The bones literally float in a sea of soft tissue (fascia). Changes in jaw position, tongue position and occlusion could thus be transmitted through fascial and muscular chains to distant sites such as trigger points and referral pain zones (e.g., occiput, C1, C2, C3 connected to the sacrum via the dura), and vice versa, as part of one global postural system.
Relevance to the Cricket Appliance
The Cricket applies light cyclic intermittent forces intended to enact change not just in isolated teeth but in the relationships to cranial bones and the whole biotgensegrity body. Under a biotensegrity paradigm, a gentle development of the maxilla (for example) is accommodated by changes in the connected tissue network (fascia) – the cranial bone positions change, zygomatic bones rotate slightly, the mandible shifts to a new position via temporal bone repositioning, and cervical posture may even alter to rebalance the head (head tilt). Rather than viewing these as separate side effects, biotensegrity views them as integrated responses to maintain equilibrium and stability. ¹⁵ Ricketts intuitively leveraged this: he noted that arch development in a growing child often led to spontaneous adjustments in tooth alignment and jaw posture without direct force on every tooth (via proper tongue positioning). ² By “releasing pressure on one site and shifting pressure at other sites,” the appliance taps into the innate biotensegrity of the craniofacial complex. ²
Ricketts also minimized the use of rigid full-arch bands in early treatment, preferring sectional mechanics that let teeth and bones find a balance under lighter forces. ², ¹⁷ This approach aligns with biotensegrity: heavy rigid appliances could “force” an unwanted configuration (risking strain concentration and exacerbating cranial strain patterns), whereas lighter cyclic intermittent forces let the system self-adjust through the tensional continuum. ¹, ⁷
Fascintegrity and Myofascial Chains
Recent expansions of the tensegrity idea include “fascintegrity,” which incorporates the liquid components (blood, lymph) into the model, and the mapping of myofascial meridians (chains of muscles/fascia running through the body). 14 For instance, the deep front line is a myofascial chain that connects the jaw’s muscles (such as pterygoids), through the neck, diaphragm, all the way to the pelvic floor and feet. ¹⁷ According to this concept, a forward head posture or jaw displacement can induce compensatory changes in lower body posture via fascial connections. In dentistry, this raises awareness that correcting a malocclusion might also alleviate certain postural problems or muscular tension patterns. Indeed, some clinicians have reported that expansion or functional appliances led to improved head and neck posture or reduced tension headaches, presumably by normalizing strain in the myofascial network. While evidence is mixed, some associations have been documented: e.g., children with retruded jaws often exhibit forward head/kyphotic posture, and improving the jaw position (via functional appliances) can sometimes normalize the head posture.18 This is in sync with biotensegrity – change one part of the tension network and the rest responds.
Evidence in Orthodontics
A 2020 review by Bordoni and Myers emphasizes that fascia (solid and liquid) plus tensegrity models are crucial for understanding posture and movement. ¹⁴ They note that fascia can transmit tension across long distances, meaning a localized intervention (like an oral appliance) may have system-wide effects. ¹⁹ In reviewing orthodontic research, some studies have sought to correlate occlusal traits with posture. A systematic overview (Michelotti et al., 2011) found some associations – for example, certain malocclusions related to altered head or spine posture – but it cautioned that cause-effect is not firmly established. ²⁰ However, another clinical study in children found a significant correlation between a low SNB angle (mandibular retrognathia) and kyphotic (hunched) body posture. ¹⁸ Moreover, those children with airway obstruction (enlarged adenoids) had a higher prevalence of kyphotic posture, linking craniofacial structure, airway, and whole-body alignment.¹⁸ When a Cricket appliance develops the maxilla and opens and tones the airway via improving tongue posture, it could therefore also encourage a more upright posture by alleviating nasopharyngeal blockage (thus the child no longer needs to tilt the head to breathe). ¹⁸ The tensegrity model helps conceptualize these multi-region improvements as part of one biomechanical system returning to balance.
Summary
Biotensegrity provides a biomechanical rationale for the holistic effects seen with Cricket appliances. It suggests that rather than acting on teeth alone, the appliance introduces light intermittent cyclical forces that the entire craniofacial-body system redistributes via biotensegrity, mechanotransduction and fascia, yielding changes in bone positions, soft tissue tensions, and posture that complement the dental corrections. Appreciating and understanding these concepts can guide clinicians to use Cricket appliances in conjunction with physiotherapy, breathing exercises, or body posture work, aiming for optimal systemic balance.
Fascial Dynamics and Craniofacial Orthopedics
Concept Overview
The fascial system is the continuous web of connective tissue with no beginning or end, enveloping bones, teeth, muscles, tendons, ligaments, nerves and organs. It has both superficial and deep layers, and it plays a dynamic role in transmitting mechanical forces and providing proprioceptive feedback. Fascial dynamics refers to how this network moves, adapts, and can become restricted or released. In dentistry, fascial considerations have gained attention because head, neck, and jaw structures are invested in fascia that connects to the rest of the body (as noted with myofascial chains above). Chronic malocclusion or TMJ dysfunction can lead to strain in certain fascial planes (e.g., tightness in the suprahyoid muscles’ fascia), while conversely, fascial tightness in the neck or shoulders can reflect on jaw position. Techniques like craniosacral therapy or myofascial release are sometimes used adjunctively to ease restrictions in cranial sutures or muscles to facilitate dental changes. ¹⁴, ¹⁶
Cricket Appliance Influence on Fascia
The Cricket appliance, by changing the position of bones and teeth, inevitably applies new tension to the fascia. For example, advancing the mandible (as in Class II correction) stretches the muscles and fascia of the suprahyoid area and floor of mouth. Over time, this can strengthen and adapt those structures, which might have been functionally shortened in a retrognathic posture. Likewise, developing the maxilla not only moves cranial bones but also stretches the palatal mucosa and the attached periosteum – a fascial layer covering bone. This could stimulate fibroblast activity and new collagen deposition as part of the adaptation. A study on ALF (Advanced Light Wire Functional) appliances, which are very light wire developers, reported correction of both facial and postural asymmetry in a 12-year-old patient, attributing success in part to relieving cranial and fascial strains.²³ The ALF, a direct descendent of the Cricket, also utilizes light wire philosophy by applying light intermittent forces; the authors noted improved facial symmetry and head posture after treatment, implying that the facial fascia and musculature repositioned along with the dental changes.²³
The fascia also houses many proprioceptors and stretch receptors. As teeth move and jaws reposition, these receptors fire, sending signals to the central nervous system about the new jaw relationships. Over the course of treatment, the patient’s neuromuscular system “learns” the new correct position as the fascia/muscle tension balances out. This is why retention and stability in orthodontics often depend on a period of neuromuscular adaptation – essentially, the fascial and muscular elements must settle into the new equilibrium to hold teeth in place with the help of tongue posture, which is critical. ²⁰
Interdisciplinary Approaches
Modern practitioners sometimes collaborate with osteopaths or physical therapists when treating complex cases with appliances. An appliance might be used in conjunction with exercises that target cervical and jaw musculature or with myofunctional therapy (which trains the tongue posture and orofacial muscles). The underlying logic is to engage the fascial and muscular system in support of the skeletal changes. For instance, a narrow maxilla often correlates with a high-arched palate and a low tongue posture (the tongue not resting in the palate). The low tongue, in turn, is part of a fascial and muscular pattern that can involve a forward head posture and neck muscle strain. This also affects the tone of the airway. By developing the maxilla (with a Cricket, OLC), we create room for the tongue to rise, and concurrently teaching the patient proper tongue posture can reinforce this development. This synergy ensures that the fascia and muscles (like the tongue’s connections to the palate via the palatal aponeurosis, and to the hyoid via lingual fascia) adapt to support the new dental arch form. ¹⁴, 35
Evidence and Clarity
It must be noted that while many clinical observations support fascial involvement, rigorous scientific evidence is still developing. A critical review in Progress in Orthodontics noted that performing orthodontic treatment solely to address posture or vice versa is not yet evidence based. ²⁰ However, it acknowledged that “some associations have been found between occlusal factors and postural alterations”. ²⁰ Rather than viewing this as a direct cause-effect, it may be that certain patterns of malocclusion and body posture share common developmental origins or reciprocal influences. What is clear is that a comprehensive approach to a patient – evaluating not just teeth alignment but also breathing patterns, head position, cervical spine alignment, and even gait – can reveal patterns that recognize and dictate treatment. Ricketts was ahead of his time in this regard, considering “the future size and form of the face” and even overall patient growth in treatment planning. ² His visual treatment objective (VTO) process would predict where jaws should be at maturity and guide appliance therapy accordingly, inherently an integrative outlook.21
In Practice
Acknowledging fascial dynamics means that adjusting an appliance more gradually will allow soft tissues to adapt and incorporate exercises or adjunct therapies to relieve any strain. It embodies the principle “primum non nocere” (first, do no harm) by ensuring that as we allow cranial facial system to unwind and reposition, we are not creating unintended stress elsewhere – i.e., Biotensegrity. The result is a more comfortable treatment and often a healthier overall outcome, with patients experiencing improvements in not just facial muscle tension or even breathing, but the whole body. In Biotensegrity, if one part of the body is affected, the rest of the body is too. ¹⁴
Cranial Bone Posture and Sutural Adaptation
Concept Overview
The human skull is composed of numerous bones joined by sutures—fibrous joints that allow a tiny degree of movement and growth. Cranial bone posture refers to the positional relationships of those bones (e.g., how the maxillae is connected to the palatines bones, sphenoid bone and occiput etc.). The human skull consists of twenty-nine bones: eight cranial bones, fourteen facial bones, and seven additional bones including those of the inner ear and the hyoid bone. Cranial bone movement is dictated by sutural anatomy and by pressure from the cerebrospinal fluid (CSF), which circulates throughout the spinal cord and brain within the dura mater. CSF is critical for oxygenation and nourishment of the brain and spinal cord, eliminating toxins and cooling the pituitary and hypothalamus, which regulate hormones. ²²
The cranial bones are classified as paired or midline, depending on whether they cross the midline. In early development, cranial sutures are highly malleable, permitting skull expansion and contraction to accommodate brain and facial growth. Traditionally, it was thought that sutures fuse by late adolescence, rendering bone positions fixed. However, evidence suggests most sutures (e.g., the midpalatal suture and some at the cranial base) retain remodeling capacity into adulthood. ²²
Ricketts Appliance and Cranial Sutures
During Ricketts’ era, adult expansion without surgery was rare. However, in growing patients, Ricketts strongly advocated sutural expansion. He described how quad-helix or activator appliances influence not only tooth alignment but maxillary and mandibular growth relative to the cranial base.² Expanding the maxilla stresses circummaxillary sutures (connecting the maxilla to the palatine, zygomatic, temporal, and sphenoid bones), allowing the maxilla to “uncouple” slightly and adopt a broader posture. Cephalometric studies show that orthopedic expansion in youth can produce slight “disimpaction” of the maxilla, with downward and forward movement that may improve Class III relationships or increase airway volume. ²
Ricketts also utilized high-pull headgear to redirect maxillary growth relative to the cranial base, another example of orthodontic modulation of cranial bone posture. ² Modern CBCT studies confirm that rapid maxillary expansion separates not only the midpalatal suture but also adjacent cranial sutures (e.g., zygomatico-maxillary, fronto-maxillary) and slightly opens the pterygoid plates from the sphenoid. ²² This confirms cranial bones are not rigidly immobile; dental appliances can modify their relationships. It needs to be noted with caution that if malposition cranial bones are not allowed to be freed up before the expansion occurs the cranial strains can be exacerbated.
Osteopathic concepts of cranial strain patterns suggest that even adults exhibit subtle cranial bone micro-mobility tied to the breathing cycle, susceptible to maladaptive “strain patterns” after trauma, aggressive orthodontics, or chronic dysfunction. Lightwire or functional appliances (OLC) have been shown to relieve such cranial distortions by balancing asymmetric forces in the mouth and face. 35 Another clinical example is the ALF case report by Strokon (2010) demonstrating improved dental alignment accompanied by increased cranial symmetry visible on radiographs. ²³
Airway and Cranial Posture
Cranial bone posture notably affects airway dimensions. A retruded maxilla or high-arched palate (common in long, narrow faces) reduces nasal cavity volume, increasing nasal airflow resistance because the palate forms the floor of the nasal cavity. Altering maxillary posture by expansion and advancement enlarges the nasal cavity. ²⁴ Singh et al. (2016) demonstrated significant nasal cavity volume increase in adults after biomimetic oral appliance therapy (from ~42 cm³ to ~44 cm³ on average), corresponding to subtle cranial bone repositioning that widens the nasal floor and lateral walls, thereby facilitating nasal breathing. ²⁴
Ricketts noted that slow palatal development in youth widens the nasal cavity and prevents mouth-breathing, which is associated with open-mouth and forward-head posture compensations that negatively affect jaw, hyoid, and cervical spine relationships.² Addressing cranial bone posture through appliances that develop the palate and advance the mandible can break this vicious cycle, improving posture, tongue positioning, airway, and neurological function.
Cranial Base Angles
Ricketts’ cephalometric analysis included assessing cranial base angles (e.g., saddle angle), which influence jaw relationships. Appliance therapy may induce adaptive growth changes at synchondroses (cartilaginous joints in the cranial base). For instance, Class III correction combining expansion and chin cup might slightly increase the cranial base angle, mitigating mandibular prognathism tendencies. Iwanicki et al. (2022) reported successful camouflaging of mild Class III malocclusion with asymmetry using Ricketts’ non-surgical approach, implying orthopedic jaw positioning favorably influenced cranial base growth. ²¹
Summary
Cranial bone posture is both an influencer and target of the Cricket appliance. Correct appliance application can improve cranial strain patterns detrimental to systemic health by harnessing remaining sutural growth or inducing adult sutural adaptation. This results not only in occlusal improvement but also enhanced airway dimensions and a balanced craniofacial complex with potential neurological benefits, exemplifying the interdisciplinary orthodontic approach championed by Ricketts. ²
Airway Influences of the Ricketts Appliance
Concept Overview
The relationship between craniofacial posture, the upper airway, and neurology is becoming increasingly central in dentistry and sleep medicine. Constricted dental arches, retrognathic jaws, or high palates can narrow the airway, contributing to obstructive sleep apnea (OSA) by reducing nasal or pharyngeal space.²⁴ Conversely, jaw development or advancement often improves airway patency. Airway-focused orthodontics, sometimes called pneumopedics, utilizes appliances to remodel airway-supporting structures. Since there are twelve cranial nerves that exit through the cranial bones, it stands to reason the wedged, restricted malpositioned cranial bones have a direct effect on their function (i.e. five cranial nerves go through the sphenoid bone alone).
The Cricket appliance inherently affects the airway: by developing the palate, it enlarges the nasal floor; by advancing the mandible (as in Class II correction or OSA devices), it increases pharyngeal airway space. This anterior mandibular positioning allows the tongue a more forward posture, enhancing airway tone, size and neurology via Vagus( X) nerve activation.
Evidence of Airway Improvement
Numerous studies and meta-analyses confirm that rapid maxillary expansion (RME) alleviates nasal obstruction and mild pediatric OSA. ²⁵ A recent systematic review (Hariharan et al., 2025) found RME effective in reducing apnea-hypopnea index (AHI) and improving oxygen saturation in both pediatric and adult OSA patients. Especially in children with maxillary deficiency, RME often resolves OSA, validating it as a genuine pediatric treatment. ²⁵ The mechanism involves widening the nasal cavity and improving tongue posture by expanding palatal space.
However, relapse can occur in approximately 40% of cases, underscoring the importance of considering and addressing cranial bone posture initially. If maxillary expansion improves airway volume but cranial strain patterns remain untreated, systemic balance may worsen, negatively affecting overall health and exacerbating the existing cranial strain pattern.
In adults, combining mandibular advancement with expansion represents a new frontier. The Ricketts phonetic bite method helps locate the individual’s optimal mandibular forward position to maximize airway openness. ² Mandibular advancement devices (MADs) built using this position effectively reduce snoring and mild-to-moderate OSA by pulling the tongue and soft tissues forward, enlarging the retroglossal airway. ²⁶ MADs can reduce AHI by approximately 50% in suitable patients and improve nocturnal oxygen saturation. ²⁶
Airway-Appliance Interaction
The Cricket appliance’s influence on jaw morphology impacts airway health long-term. Maxillary development in children promotes nasal breathing and proper craniofacial growth by encouraging tongue-palate contact and forward facial growth. ² Ricketts advocated arch development and non-extraction approaches partly to maintain airway space, as extractions in high-angle, small mandible cases can exacerbate airway constriction. ² Functional appliances like the Cricket, by posturing the mandible forward during growth, increase pharyngeal airway dimensions. ²⁴
Cephalometric studies show that after 12+ months of functional appliance therapy, upper airway space behind the soft palate increases in teens. Early airway intervention can break mouth breathing cycles, preventing maxillary constriction and mandibular retrusion.
Quantitative Insights
Singh et al. (2016) observed a ~5% nasal volume increase in adults following approximately 18 months of Biomimetic Oral Appliance Therapy²⁴. Additional studies report modest increases in nasal valve area and decreases in nasal resistance following RME in children. ²⁵ Villa et al. (2011) demonstrated that pediatric OSA improvements from RME persist two years post-treatment, suggesting durable orthopedic airway benefits. ²⁵
Imaging clearly shows these changes: pre- and post-treatment CBCT scans display a widened nasal floor and more parallel nasal cavity walls; lateral cephalograms reveal increased superior oropharyngeal airway space when mandibular advancement devices are in place.
Conclusion
Airway improvement is a crucial benefit of the Cricket appliance within a dentist’s therapeutic armamentarium. Treatment planning that prioritizes aesthetics, occlusion, airway function, and cranial strains aligns with Ricketts’ comprehensive care ethos. Palatal expansion in growing patients and mandibular positioning in adults enjoy strong evidence for airway benefit. ²⁴, ²⁵
Neurological Signaling and Mechanotransduction in Appliance Therapy
Concept Overview
The Cricket appliance induces changes by engaging both the nervous and skeletal systems. Neurological signaling occurs on multiple levels: (1) peripheral mechanoreceptors and proprioceptors sensing forces and tooth movements, (2) central processing of these signals modulating muscle activity, and (3) cellular signaling pathways, which intersect with neural inputs via neuropeptides and neurotransmitters. ²⁸
The periodontal ligament (PDL) and temporomandibular joint (TMJ) are richly innervated with mechanoreceptors (such as Ruffini endings and periodontal pressoreceptors) detecting pressure and stretch, alongside nociceptors sensing pain from excessive force. ²⁸ When an appliance applies force, these receptors transmit information about force magnitude and direction to the trigeminal nucleus in the brainstem. ²⁹ Reflex arcs adjust jaw muscle activity accordingly—for instance, excessive force can trigger nociceptive reflexes that reduce masticatory muscle activity to protect teeth, while properly calibrated forces enhance proprioception and muscular coordination. ²⁸ Reflex arcs then influence jaw muscle activity – for instance, heavy orthodontic force or a high bite can trigger a nociceptive reflex reducing masticatory muscle activity to protect the teeth (this is akin to a jaw-opening reflex). Conversely, a well-tuned appliance like the Cricket can stimulate proprioceptors in a way that enhances muscular coordination and tone. The body will respond to forces that are desirable and natural not forced.
Mechanotransduction at the Cellular Level
Mechanotransduction describes how cells convert mechanical stimuli into chemical signals. In orthodontics, PDL cells and osteocytes sense mechanical strain and release signaling molecules mediating bone remodeling. ²⁸ The Piezo1 ion channel, a mechanosensor in PDL cells, opens in response to stretching, allowing calcium influx and triggering bone formation cascades on the tension side. ²⁸ Jiang et al. (2021) showed that blocking Piezo1 in an animal model reduced orthodontic tooth movement and was associated with lower expression of osteogenic factors like RUNX2 and Osterix. Blocking Piezo1 reduces tooth movement and osteogenic factor expression, confirming its role in transducing mechanical forces into biological responses. ²⁸ This confirms that the mechanical force from an appliance is sensed and transduced by specific cellular pathways, which then orchestrate the deposition or resorption of bone necessary for tooth movement. Notably, some of these pathways involve neurological molecules too: PDL cells and osteoblasts can release neurotransmitter-like substances (e.g. ATP, nitric oxide) upon mechanical stimulation, which modulate blood flow and nerve activity in the area. ²⁹
Trigeminal Nervous System Effects
The trigeminal nerve (cranial nerve V) is the primary sensory nerve for the face and jaws. It has extensive connections in the brainstem (trigeminal nucleus) which is linked to the autonomic nervous system and pain modulatory systems. Chronic static orthodontic forces or a new mandibular position can alter trigeminal input patterns. This can have seemingly unrelated effects such as changes in body posture (through trigeminal-cervical reflexes) or even cardiovascular responses (through trigeminal-parasympathetic reflexes). For example, it’s documented that stimulation of trigeminal afferents (like cooling the face or pressure on teeth) can cause reflex bradycardia – the so-called trigeminal cardiac reflex. ²⁸ While we traditionally think of an orthodontic appliance is a benign stimulus, it still constantly feeds information to the brain about jaw position. Over time, a new occlusion “feels normal” to the patient as the sensory cortex adapts to the new proprioceptive inputs. ²⁸
Functional appliances in growing patients not only reposition jaws but retrain neuromuscular patterns. Electromyographic studies show changes in resting masticatory muscle activity after Herbst or twin-block treatments, indicating improved muscle tone symmetry and coordination. ²⁸ Ricketts observed that improved occlusion (e.g., aligning incisors, correcting overbites) often reduces jaw fatigue and headaches, reflecting neural and muscular harmony. This is partially a neural effect: muscles were firing more symmetrically and efficiently after treatment, reducing strain.
Pain and Inflammation Signaling
One cannot discuss neural aspects without mentioning pain. Orthodontic tooth movement does cause transient inflammatory pain – typically one or two days after an adjustment, patients feel soreness due to PDL inflammation. This involves nociceptive neurons releasing neuropeptides like substance P and CGRP (calcitonin gene-related peptide) in the PDL, which increase blood vessel permeability and recruit immune cells. Interestingly, these same neuropeptides also influence bone remodeling: CGRP, for instance, can enhance osteoblastic activity. Nociceptor signaling via the trigeminal nerve thus might directly modulate the rate of tooth movement, an area of ongoing research. ²⁹ If an appliance is adjusted too aggressively and causes excessive pain, the heightened nociceptive input could paradoxically slow tooth movement by inducing a stronger inflammatory response and causing patient to chew differently (avoiding bite, etc.). Ricketts was aware of managing patient comfort – his light-force approach minimized pain, which not only is kinder to the patient but potentially more physiologically efficient for movement (since extreme pain/inflammation is not optimal for controlled remodeling). ²⁹
Central Integration
Brain plasticity allows prolonged occlusal changes to reshape somatosensory cortex representations of the jaw and teeth. Functional MRI and somatosensory evoked potential studies confirm cortical remapping after orthodontic treatment. ²⁸ Appliances such as the Gelb or Tanner splints help reduce parafunctional muscle activity by neuromuscular reprogramming.²⁸ Cranial strain patterns significantly impact TMJ health; uncorrected temporal bone misalignment can perpetuate pathology even after occlusal adjustments.²⁸
Summary
The Cricket appliance influences a broad neurological signaling spectrum: from Piezo1-mediated mechanotransduction in PDL cells to trigeminal reflexes modulating muscle tone and cortical plasticity adapting to a new bite. Precision and gradual adjustments are vital to harness favorable neural responses, ensuring stable and comfortable treatment outcomes supported by the patient’s neuro-musculoskeletal system. By leveraging favorable neural responses (like enhancing proprioceptive input for stability and minimizing nociceptive input), the appliance can achieve stable and comfortable results that the patient’s nervous system will help maintain.
Facial Asymmetry: Diagnosis and Appliance-Based Correction
Concept Overview
Facial asymmetry includes dental midline discrepancies, jaw size or positional differences between sides, cranial bone malpositioning, posture issues, airway restrictions, neurological dysfunction and muscular imbalances. Causes may include unilateral crossbites, habitual postures, or developmental anomalies. It is essential to differentiate between dental asymmetry (teeth misaligned within symmetric jaws) and skeletal asymmetry (unequal jaws or cranial base) for effective treatment planning. ³³
Ricketts emphasized early treatment of unilateral crossbites—using appliances like the quad-helix or expansion plates—to prevent functional mandibular shifts that can cause asymmetric growth. ³¹ His records routinely incorporated lateral photographs and frontal cephalometric analyses to assess asymmetry, highlighting the need for individualized, side-specific force application during therapy. ³¹
Clinical Evidence
Strokon’s 2010 case report using the Advanced Lightwire Functional (ALF) appliance detailed correction of a facial asymmetry associated with cranial torsion. Besides dental improvement, the case demonstrated enhanced facial symmetry and head posture, suggesting the appliance’s effect extended beyond teeth to muscular and skeletal systems. ³² While such case studies are low-level evidence, they illustrate the potential for functional appliances to influence overall facial balance.
Treatment Strategy
Successful facial asymmetry correction with Cricket appliances relies on light intermittent cyclical forces, removing obstacles and creating gaps or spaces to allow the body to achieve more balance and function. Understanding individual growth patterns and skeletal discrepancies enables clinicians to customize appliance adjustments rather than using uniform force protocols. ³¹ This approach aligns with Ricketts’ patient-centered philosophy, focusing on the unique biomechanical needs of each patient.
Recent literature supports that, with careful execution, removable functional appliances can harmonize facial symmetry and occlusion without surgical intervention. ³¹ These findings validate the comprehensive, interdisciplinary framework pioneered by Ricketts, reinforcing the appliance’s capacity to address complex asymmetries.
Summary
Facial asymmetry correction with Cricket appliances is feasible and effective when guided by precise diagnosis and individualized force management. Integrating cephalometric and photographic analyses into treatment planning enables clinicians to correct skeletal and dental discrepancies while promoting improved balanced muscle function, posture, airway and neurology. The approach exemplifies the logical and integrative orthodontic philosophy that underpins the Cricket appliance system. ³¹
Conclusion
The Cricket oral appliance framework stands as a testament to interdisciplinary orthodontics – an approach that transcends mere tooth alignment to engage growth biology, physics, and whole-body health. In this review, we explored how a single appliance system can interweave with epigenetic mechanisms, harnessing gene-environment interplay to unlock latent developmental potential. 8 We saw that by acknowledging principles of quantum biology, such as piezoelectric signaling in bone, we gain an appreciation for the deep physical processes an orthodontic force can initiate. 10 We affirmed that the craniofacial system operates on a model of biotensegrity, wherein an adjustment in one part (like maxillary expansion) redistributes tension throughout the connected musculoskeletal network. 14 We examined fascial dynamics, noting that the success of orthopedic corrections often depends on the adaptive capacity of soft tissue and the reprogramming of muscle patterns.19 The appliance’s effect on cranial bone posture and airway was highlighted by evidence of suture expansion improving nasal breathing and pharyngeal space. 2 We delved into neurological signaling, from mechanotransduction in PDL cells to reflexes and central plasticity, which collectively ensure that the changes wrought by the appliance are integrated and stabilized in the patient’s nervous system. 11 Finally, we addressed facial asymmetry, demonstrating that meticulous appliance design and force management can successfully correct imbalances, yielding symmetric form and function. 31
Through detailed protocols, we translated these concepts into actionable steps, emphasizing “irrefutable logic” at each stage – such as widening a narrow palate to remove functional matrix constraints on nasal breathing (a logical cause-effect supported by literature) or incrementally advancing a jaw to allow neuromuscular adaptation (respecting biologic limits to ensure precision in outcome). The use of high-quality sources from orthodontics, sleep medicine, and anatomy strengthened each argument: for instance, citing the meta-analysis confirming RME’s efficacy in OSA 31, or the Cureus review on fascia underlining how global the impact of local interventions can be. 14
In conclusion, the Cricket appliance is not an obsolete relic but rather a versatile and valuable part of the armamentarium for natural holistic whole-body treatment. It embodies dentistry’s evolution into a truly integrative discipline – “reinforcing the idea of dentistry as a medical discipline requiring interdisciplinary effort,” as recently noted in an Angle Orthodontist tribute to Ricketts.1 By building on Ricketts’ foundation with contemporary knowledge, clinicians can achieve results that are stable, health-promoting, and grounded in the fundamental workings of biology. The logic is straightforward: treat the root cause, guide growth, respect the body’s networks and the results will follow. Precision is ensured by constant reference to scientific metrics and feedback loops during treatment. As we carry this legacy forward, future research (perhaps on molecular genetic changes during such therapies, or finite element models incorporating tensegrity) will further validate and refine the principles, but the existing evidence and successful outcomes already position the Ricketts approach as a paradigm of evidence-aligned innovation in orthodontics.
Current Developments Utilizing the Cricket Appliance
Dr. Ricketts introduced the Cricket appliance in the mid-1980s as an advanced orthodontic technique. He claimed it could straighten teeth fully without other appliances, suggesting it could sometimes replace braces by developing arches and correcting tooth rotations and angulations. ² Despite its theoretical advantages, the Cricket was technically demanding to fabricate and adjust, requiring high-level orthodontic laboratory skill, limiting widespread adoption. ²
Only master technicians like David Gergen, who worked closely with Ricketts, routinely fabricated the appliance, further restricting its popularity. ² Over time, the Cricket was overshadowed by more user-friendly fixed expanders and functional appliances fitting conventional orthodontic practice models better.
Published clinical research on the Cricket appliance is limited to case reports and expert opinion. It functions as a hybrid of the quad-helix and Crozat appliances, producing arch development and orthopedic effects in growing patients. ² Modern clinicians may use variants of its principles, such as removable spring aligners, Crozat-like appliances, ALF appliances, and OLC particularly in holistic and airway-focused practices.
West’s 1984 article demonstrated successful adult treatment cases with the Cricket, showing efficacy for adults refusing fixed appliances or with minor malocclusions² . Its design allows a variety of tooth movements, including rotation, torque, and molar distalization, enabling sagittal corrections and vertical settling ².
The Cricket had been largely a historical footnote that served as a precursor to contemporary removable functional appliances. Its legacy lied in proving that comprehensive orthodontic corrections with removable devices are possible, emphasizing arch development to avoiding extractions. This philosophy aligns with many modern functional orthodontic approaches. Until now its use has been limited and stymied for the above noted reasons. For this reason, I have reintroduced the basic Cricket appliance and all its fantastic attributes and modified it naming it the Open Loop Cricket (OLC).35
What is new?????
Introducing the Open Loop Cricket (OLC):
The Open Loop Cricket (OLC) 35 is a new concept merging holistic principles to unwind cranial strain patterns while moving with fascial dynamics, improving posture, airway and neurology. The human skull consists of twenty-nine bones: eight in the cranial system, fourteen in the facial group, and seven comprising the inner ear and the hyoid bone. The cranial bones have movement dictated by their sutural anatomy and pressure from the cerebral spinal fluid (CSF), which circulates throughout the spinal cord and brain within the dura’s confines. CSF is critical for oxygenation and nourishment of the brain and spinal cord, toxin elimination, and cooling of the pituitary and hypothalamus, vital for hormone regulation.
The cranial bones are classified as paired or midline bones depending on whether they cross the midline. Visually, the face’s skin is supported by fat pads and cranial bones. Removing skin and fat reveals cranial bone asymmetry patterns translating to facial asymmetry. Various factors, such as fetal positioning in the pelvic girdle, birth canal passage, C-sections, diet, and breastfeeding absence, can influence cranial bone positioning and craniofacial asymmetry.
Dentists, focusing on the oral cavity, often overlook the maxilla’s connection to the rest of the body. The maxilla, a paired bone, connects to paired palatine bones, which interlock with the sphenoid bone. The sphenoid bone acts as the central cog of cranial bones, shaped like a swallowtail butterfly with greater and lesser wings; its greater wings form the back of the orbit of the eyes (ocular asymmetry). Since the sphenoid is the central cog to the cranial bones, the maxilla can impact it indirectly via the palatine bones. Leveling the maxilla can affect how the cranial bones support and function in the whole body.
Instead of treating pain points, go to the source of pain.
The Open Loop Cricket appliance is designed to allow cranial bone positional changes alongside light wire activation. The body is a closed-loop kinematic skeletal chain with two openings: the feet arches and the bite. Teeth contact during swallowing (2,000–3,000 times daily) closes or locks this loop. This closure locks the entire skeletal system, so adjustments to cranial bones risk being counteracted at each swallow cycle. Dr. Bob Walker’s lectures highlight the dentists’ role in unlocking restricted cranial bones, influencing facial asymmetry, posture, airway, tongue position, and neurology.
Since posture dictates airway and neurology, improving facial asymmetry can alleviate and help TMD, airway and neurologic symptoms.
The benefits of the Open Loop Cricket:
Holistically moves with the fascia and the body’s cyclic intermittent motion.
Helps to improve the craniocervical junction, influencing Class I, II, III malocclusions.
Unwinds and decompresses facial cranial strain patterns (asymmetry) by creating a gap.
Enhances growth and development by optimizing whole-body function 24/7.
Addresses malocclusions root causes, often involving tongue posture.
Decompresses and realigns the TMJ complex, including temporal bone repositioning.
Enhances neurology by freeing cranial nerve pathways and improving tongue movement, supporting airway tone and vagus(X) nerve activation.
Improves posture and airway by affecting head tilt and cervical stability.
Unlike traditional mechanical expanders limited to two-dimensional palatal changes, the OLC promotes three-dimensional development influenced by tongue posture and fascial motion that allows a natural physiological growth and cranial rhythm function. The OLC’s flexible cobalt wire and acrylic component facilitates cranial bone unwinding and improved cranial nerve function, enhancing airway tone via glossopharyngeal and vagus nerve stimulation. It promotes craniocervical complex changes and improves tongue position and function, achieving stable permanent changes in occlusion, posture, airway, and neural integration.
The appliance’s goal is to restore and rehabilitate the craniofacial cervical complex’s physiological function—head, face, and neck—optimizing 24/7 bodily function.
The OLC’s wire design features a balanced for strength and flexibility, promoting facial growth, cranial motion, rhythm, and tooth position changes. Its biocompatibility with craniofacial structure and fascia cyclic motion allows synergistic movement. A gap created by an acrylic pad permits cranial bones to unwind to natural positions on mouth closing, improving facial symmetry. Cranial nerve function is enhanced by better cranial bone positioning.
Besides stimulating normal maxillary-mandibular growth, the OLC increases airway space and tone, crucial for the tongue’s anterior and superior mobility. This tones the airway via glossopharyngeal and palatoglossal muscles activation by the vagus nerve.
Unlike rapid palatal expanders, which develop the palate in two dimensions (potentially worsening cranial strains), the OLC develops the palate in three dimensions via tongue function and passive qualities, restoring function while facial structures evolve.
The objective is to remove obstacles, restore inherent bodily motion and function, creating maximum capacity and space for transformation. This facilitates healing by engaging natural body rhythms, encouraging openings and gaps to release cranial strains and fascial restrictions.
In summary, the OLC embodies a holistic, biomechanical, and neurological approach to orthodontics, restoring craniofacial function, posture, airway, and neurology by removing obstacles and augmenting the body’s inherent motion and healing capacity.
Final Thoughts: Motion is inherent in living systems; restoring it should be our goal. The OLC increases motion while restoring function, addressing malocclusion and craniofacial asymmetry causes. Healthcare providers aim to remove obstacles, augment motion, and restore health. Restoring cellular and cranial motion and proper breathing enables the body to self-heal.
References